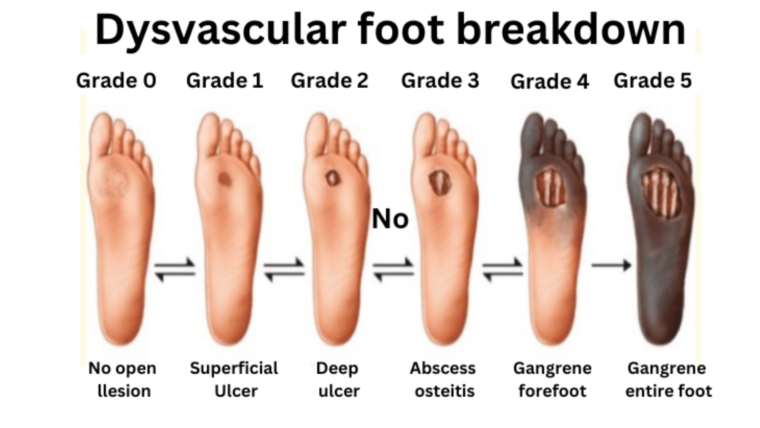
Advanced diabetes, also known as end-stage diabetes, can be detected by clinical and laboratory diagnostics. The technique for diagnosing diabetes entails monitoring the patient’s blood sugar levels and looking for diabetic complications. To diagnose advanced diabetes, various tests can be performed, including the Hemoglobin A1C (HbA1C) test, which measures the average blood sugar level over the previous two to three months, the fasting blood glucose test, which measures the blood sugar level after an overnight fast, the oral glucose tolerance test (OGTT), which measures the blood sugar level before and after drinking a glucose-rich beverage, and urine tests that assess the presence of ketones, which indicate poorly controlled diabetes. Furthermore, the eye exam can detect diabetic retinopathy, whereas the foot exam can identify diabetic neuropathy and other foot issues.
Following a diagnosis, the healthcare professional may offer a variety of treatments to manage the illness, such as lifestyle changes, medication, and insulin therapy.
Diabetes Classification and Diagnosis @ DiaBeat-Surat
Diabetes was initially classified into two types: juvenile-onset diabetes mellitus, now known as type 1 diabetes mellitus, and adult-onset diabetes mellitus, now known as type 2 diabetes mellitus. This has expanded to include more than 50 subcategories caused by various pathogenic mechanisms or associated with other diseases and syndromes. Diabetes diagnosis has progressed from physician recognition of typical symptoms to detection of ambient hyperglycemia and, from there, to the definition of excessive plasma glucose levels after an overnight fast and/or following a glucose load challenge (oral glucose tolerance test or OGTT), and, more recently, by measurement of glycated hemoglobin. (A1c). Diabetes screening has revealed a substantially higher prevalence of the disease in the United States and worldwide, as well as its massive public health burden. Modern testing has identified individuals who are at high risk of developing diabetes, as well as pregnant women whose foetuses are at elevated risk of mortality and morbidity.
Type 1 diabetes is caused by an autoimmune attack on the pancreatic islet beta cells, which is manifested by autoantibodies and T lymphocytes reacting with islet cell antigens both before and after hyperglycemia develops. Insulin insufficiency causes hyperglycemia and the danger of ketosis when roughly 80% of beta cells are damaged or killed. In turn, hyperglycemia produces osmotic diuresis, which results in frequent urination, thirst, and weight loss. Insulin resistance and relative insulin insufficiency combine to develop type 2 diabetes. Obesity, a sedentary lifestyle, and advanced age all contribute to insulin resistance. Obesity is now common in both adolescents and adults, and the pathogenetic variables of type 1 and type 2 diabetes overlap in many people. Gestational diabetes is unique to pregnancy and is a precursor to type 2 diabetes.
Diabetic retinopathy has been used as a distinct consequence of the disease to develop diagnostic glycemic criteria for presymptomatic diabetes: A1c of 6.5%; fasting plasma glucose (FPG) of 126 mg/dL; or 2-hour plasma glucose (PG) of 200 mg/dL determined following an OGTT. A random plasma glucose level of 200 mg/dL is diagnostic for people with usual symptoms. The 2-hour PG produces the highest frequency and the lowest A1c. A1c is the most practical and convenient test since it requires no preparation, is analytically superior, and has the lowest intraindividual variation. It costs more than the FPG but the same as or less than the OGTT. The 2-hour PG is the most taxing on the patient and has the greatest intraindividual variability. A1c is not always measured in a consistent manner. It is recommended to confirm an abnormal result with the same test.
Glycemic testing demonstrate inconsistency across populations, according to studies. 27%-98% of patients who meet the A1c criterion also meet the plasma glucose criteria. 17%-78% of patients who meet the plasma glucose threshold also meet the A1c criterion. These disparities exist because each test examines a distinct element of hyperglycemia, which varies between people. While the risk of future diabetes is always related with plasma glucose and A1c levels, the areas between the upper limits of normal and the diabetes cutpoints have been referred to as “prediabetes” or “high risk for diabetes.” A1c 6.0%-6.4% or 5.7%-6.4%; impaired fasting glucose (IFG), FPG 100-125 mg/dL; and impaired glucose tolerance (IGT), 2-hour PG 140-199 mg/dL are the categories. A1c levels of 6.0%-6.4% increase the odds ratio (OR) for diabetes progression (OR 12.5-16) greater than levels of 5.7%-6.4%. (OR 9.2).
After being diagnosed with advanced diabetes, it’s important to work closely with your healthcare provider to develop a comprehensive management plan. Here are some steps you can take:
- Follow your treatment plan: This may include lifestyle changes, such as eating a healthy diet, exercising regularly, and losing weight if necessary. It may also involve taking medication as prescribed and monitoring your blood sugar levels regularly.
- Learn how to manage your condition: This can include learning how to inject insulin if needed, how to monitor your blood sugar levels, and how to recognize and manage the signs and symptoms of hyperglycemia (high blood sugar) and hypoglycemia (low blood sugar).
- Take steps to prevent complications: This may involve regular eye exams, foot exams, and other diagnostic tests to identify and manage complications such as diabetic retinopathy, neuropathy, and nephropathy.
- Seek psychological support: Managing a chronic condition like advanced diabetes can be challenging, and it’s not uncommon to experience depression, anxiety, or other mental health issues. Psychological support from a therapist or counselor can be helpful.
- Make healthy lifestyle choices: Quit smoking, limit alcohol intake, and manage stress levels as much as possible. These lifestyle factors can all impact your diabetes management and overall health.
- Stay informed: Keep up to date with the latest research and advances in diabetes management, and stay in touch with your healthcare provider to ensure that you’re receiving the most up-to-date care.